Frequently Asked Questions (FAQs)
FAQs aimed to address some of the key questions asked about MBS item numbers used for the provision of primary mental healthcare. It includes common questions and answers obtained from various sources, such as the Australian Psychological Society (APS) and the Department of Health.
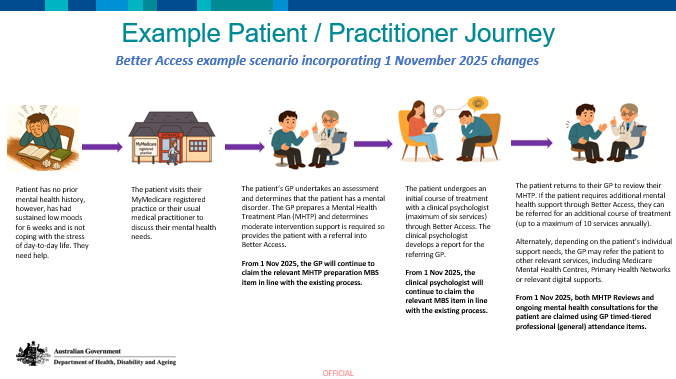
1 November 2025 changes to Better Access
From 1 November 2025, changes will be introduced to the Better Access to Psychiatrists, Psychologists and General Practitioners through the Medicare Benefits Schedule (MBS) initiative.
These changes, consistent with recommendations from the Better Access Evaluation in 2022, aim to:
- Improve equity of access to mental health supports and services.
- Strengthen the holistic relationship between patients and their healthcare providers.
- Reduce administrative burden and complexity for GPs and Prescribed Medical Practitioners by allowing greater flexibility through time-tiered general attendance MBS items for mental health treatment plan reviews, referrals, and consultations.
The updates will:
- Enhance continuity of care by linking mental health treatment plans, reviews, and referrals to a patient’s MyMedicare practice or usual medical practitioner.
- Better integrate physical and mental health care by removing specific MBS items for mental health plan reviews and consultations, enabling use of general attendance items instead.
- Provide guidance material to support best-practice referral and review processes aligned with the Australian Government’s stepped care model.
For the specific details on what the changes are that impact you, including the PDFs and fact sheets, visit MBS Online – Better Access changes from 1 November 2025.
Please see resources at the bottom of this page for more important information such as the new patient journey.General
MBS items that relate to the provision of primary mental healthcare within a general practice setting are summarised as follows:
For more information on the mental health MBS items, please visit MBS online.
|
All GPs –
not completed MHST |
VR-GPs –
completed MHST |
Non-VR GPs – completed MHST
|
|
|
Preparation of a GP MHTP
|
|||
|
Review of a GP MHTP
|
2712 |
||
|
GP MHTP consultation
|
For more information on the mental health MBS items, please visit MBS online.
Although it is not mandatory, it is strongly recommended that GPs providing mental healthcare using GP Mental Health Care items have completed appropriate mental health training as accredited by the General Practice Mental Health Standards Collaboration (GPMHSC).
GPs who have completed a GPMHSC accredited Mental Health Skills Training (MHST) will be able to access the higher schedule fee items 2715, 2717. GPs who have not completed MHST are still able to develop a GP MHTP and claim MBS items 2700 and 2701.
Appropriate mental health training can help GPs to further develop and improve their skills in diagnosing, treating and referring patients with mental illness to appropriate services.
View accredited MHST courses.
GPs who have completed a GPMHSC accredited Mental Health Skills Training (MHST) will be able to access the higher schedule fee items 2715, 2717. GPs who have not completed MHST are still able to develop a GP MHTP and claim MBS items 2700 and 2701.
Appropriate mental health training can help GPs to further develop and improve their skills in diagnosing, treating and referring patients with mental illness to appropriate services.
View accredited MHST courses.
Mental illness is a term used to describe a range of clinically diagnosable disorders that significantly interfere with an individual’s cognitive, emotional or social abilities.
Mental illnesses applicable under Better Access
Mental illnesses not applicable under Better Access*
For up-to-date information, please refer to the International classification of diseases, 10th revision (ICD-10).
*Although these are not mental illnesses applicable under the Better Access initiative, GPs can address them when patients who present with mental illness have comorbidity with one or more of these conditions (e.g. when treating a patient who has impaired cognition and mental illness)
Mental illnesses applicable under Better Access
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mental illnesses not applicable under Better Access*
|
|
|
|
For up-to-date information, please refer to the International classification of diseases, 10th revision (ICD-10).
*Although these are not mental illnesses applicable under the Better Access initiative, GPs can address them when patients who present with mental illness have comorbidity with one or more of these conditions (e.g. when treating a patient who has impaired cognition and mental illness)
Developing a GP Mental Health Treatment (GPMHTP)
A GP MHTP or mental health care plan documents the assessment, treatment, planning and review of patients experiencing symptoms of a mental illness.
A GP MHTP considers a patient’s needs, goals, action and appropriate treatment options or services for ongoing management of their mental healthcare.There is no particular form that is used for preparing a GP MHTP; however, templates are available to assist GPs. The GPMHSC have published revised versions of the GP MHTP templates. Download the revised of GP MHTP templates.
A GP MHTP is not a referral and alone is not sufficient for a psychologist, or other mental health practitioner to provide a service. For more information, see FAQs 13 and 14.
A GP MHTP considers a patient’s needs, goals, action and appropriate treatment options or services for ongoing management of their mental healthcare.There is no particular form that is used for preparing a GP MHTP; however, templates are available to assist GPs. The GPMHSC have published revised versions of the GP MHTP templates. Download the revised of GP MHTP templates.
A GP MHTP is not a referral and alone is not sufficient for a psychologist, or other mental health practitioner to provide a service. For more information, see FAQs 13 and 14.
Since a G PMHTP triggers a patient’s eligibility for funding under the Better Access initiative, a new mental health care plan should not be prepared unless clinically required.
A patient can continue on the same GP MHTP indefinitely with the GP updating a patient’s original plan over the years if appropriate. In certain circumstances, it may be appropriate for the GP to prepare a new mental health care plan. For example, if a significant change occurs with the patient’s circumstance or if a patient transfers their care to a new GP.
A patient can continue on the same GP MHTP indefinitely with the GP updating a patient’s original plan over the years if appropriate. In certain circumstances, it may be appropriate for the GP to prepare a new mental health care plan. For example, if a significant change occurs with the patient’s circumstance or if a patient transfers their care to a new GP.
Review of a GPMHTP
Under the Better Access initiative, GPs should initially refer eligible patients for six psychological services. A review of a patient’s G PMHTP should be conducted after the sixth session, after which the GP may recommend another four sessions if the patient requires further therapy.
Patients with a GP MHTP should have at least one formal review. Generally, a formal review (MBS item 2712) should occur four weeks to six months after the completion of a GP MHTP. If a further review is required, this can occur three months after the first review. Most patients should not need more than two formal reviews in a 12-month period.
For more information, including steps involved in reviewing a GP MHTP, visit the Department of Health website.
Patients with a GP MHTP should have at least one formal review. Generally, a formal review (MBS item 2712) should occur four weeks to six months after the completion of a GP MHTP. If a further review is required, this can occur three months after the first review. Most patients should not need more than two formal reviews in a 12-month period.
For more information, including steps involved in reviewing a GP MHTP, visit the Department of Health website.
Review of a GPMHTP (MBS item 2712) can also be used where a GP is managing a patient under a referred psychiatrist assessment and management plan (MBS item 291). It is also expected that MBS item 2712 would generally not be claimed within four weeks of a claim for a referred psychiatrist assessment and management plan (MBS item 291).
MBS item 2712 does not have to be used in order for additional psychological services to accessed. GPs can use a different MBS item number to conduct a review of a patient’s GPMHTP, such as attendance items 23, 36 and 44 (depending on time and context requirements).
MBS item 2712 does not have to be used in order for additional psychological services to accessed. GPs can use a different MBS item number to conduct a review of a patient’s GPMHTP, such as attendance items 23, 36 and 44 (depending on time and context requirements).
GP Mental Health care consultation item (MBS item 2713)
The GP Mental Health care consultation item applies to surgery consultations, which are at least 20 minutes duration and where the primary treating problem is related to a mental disorder.
MBS item 2713 is for the ongoing management of patients with a mental disorder, including patients managed under a GP MHTP. However, it can be used whether or not a patient has a GP MHTP.
For more information of the MBS item 2713, visit MBS online.
MBS item 2713 is for the ongoing management of patients with a mental disorder, including patients managed under a GP MHTP. However, it can be used whether or not a patient has a GP MHTP.
For more information of the MBS item 2713, visit MBS online.
There is no limit or ‘cap’ on the number of GP Mental Health care consultation items that can be claimed by a medical practitioner for services to eligible patients.
MBS item 2713 may be used for ongoing management of a patient with a mental illness and can be claimed if the patient requires an extended consultation. The item number should not be used for the development of a GP MHTP and cannot be used at the same time as the review of a GP MHTP.
MBS item 2713 may be used for ongoing management of a patient with a mental illness and can be claimed if the patient requires an extended consultation. The item number should not be used for the development of a GP MHTP and cannot be used at the same time as the review of a GP MHTP.
COVID-19 and MBS item numbers for mental health
Descriptors and rebates for the additional COVID-19 telehealth MBS item numbers are found in the Telehealth consultations section of our website.
No. GPs are not required to bulk bill the COVID-19 telehealth item numbers, unless the service provided is for Commonwealth concession card holders, children under 16 years and patients who are more vulnerable to COVID-19.
From 9 October 2020 until 30 June 2022, eligible patients with an assessed mental illness can access 10 additional psychological therapy sessions under the Better Access initiative.
In order to access these sessions, patients will be required to:
A fact sheet outlining the changes is available on MBS online.
In order to access these sessions, patients will be required to:
- have a Mental Health Treatment Plan
- have used all of their 10 sessions in a calendar year
- undertake a review of their plan with their GP after the tenth session.
A fact sheet outlining the changes is available on MBS online.
GPs who are registered as FPS providers with Medicare Australia, can claim six new item numbers for the provision of FPS services. There are both face-to-face and telehealth (video and phone).
Descriptors and rebates for the new FPS item numbers are found in the Telehealth consultations section of our website.
Descriptors and rebates for the new FPS item numbers are found in the Telehealth consultations section of our website.
Patient Eligibility
The Better Access initiative allows eligible patients with an assessed mental illness to access 10 individual psychological therapy sessions per calendar year.
From 9 October 2020 until 30 June 2022, eligible patients can receive 10 additional individual psychological therapy sessions per calendar year. The change will expand availability of these additional 10 sessions nationally to eligible people whose mental health has been adversely impacted by COVID-19.
From 9 October 2020 until 30 June 2022, eligible patients can receive 10 additional individual psychological therapy sessions per calendar year. The change will expand availability of these additional 10 sessions nationally to eligible people whose mental health has been adversely impacted by COVID-19.
From 9 October 2020 until 30 June 2022, the maximum number of Medicare funded services per calendar year under the Better Access initiative is 20 individual sessions. There are no exceptional circumstances that allow further services once these have been completed.
Referral for the provision of psychological services do not have an expiry dates. These services are valid for the stated number of sessions on the referral rather than a specified period.
When referred psychological services are not used during the calendar year in which the patient is referred, the unused services may be used the next calendar year. In this instance, the psychological services will count towards the maximum number of services available to the client in that year.
When referred psychological services are not used during the calendar year in which the patient is referred, the unused services may be used the next calendar year. In this instance, the psychological services will count towards the maximum number of services available to the client in that year.
Referring Patients
Patients may be referred for treatment and services under normal GP referral arrangements at any time. This can be done using MBS item 2712 (review of GP MHTP), item 2713 (GP Mental Health care consultation) or a standards consultation item. For more information, see section ‘Review of the GP Mental Health Treatment Plan.
In addition, eligible patients may also receive up to 10 group therapy services in a calendar year. The maximum of 10 group services may include psychological therapy services, FPS, allied mental health services, or a combination of these.
In addition, eligible patients may also receive up to 10 group therapy services in a calendar year. The maximum of 10 group services may include psychological therapy services, FPS, allied mental health services, or a combination of these.
It is a mandatory requirement and best practice for GPs to provide a letter when referring a patient for a psychological service. A GP MHTP alone is not considered as a referral and therefore not sufficient for the psychologist to provide a service.
According to the MBS, the referral may be in the form of a letter or email to an eligible allied health professional signed and dated by the referring practitioner. The allied health professional (i.e. psychologist) must be in receipt of the referral at the first consultation. Under the Better Access initiative, the allied health practitioner can assume the referral is for six sessions if not specified otherwise.
The revised GP MHTP templates now include a Request for services letter. This letter template can be used when referring a patient for a psychological service.
A referral letter directed to the psychologist by name or may be addressed generically to ‘the psychologist’. According to advice from Medicare, legislation does not require that a referral should be addressed to a named health professional. If a referral is addressed to one provider, the patient is not obliged to go to the same practitioner. The patient can see another practitioner in the same discipline, provided they can provide the same psychological service.
For more information on communication requirements between referrers and providers of mental health services, refer to the Practice guide: Communication between medical and mental health professionals.
According to the MBS, the referral may be in the form of a letter or email to an eligible allied health professional signed and dated by the referring practitioner. The allied health professional (i.e. psychologist) must be in receipt of the referral at the first consultation. Under the Better Access initiative, the allied health practitioner can assume the referral is for six sessions if not specified otherwise.
The revised GP MHTP templates now include a Request for services letter. This letter template can be used when referring a patient for a psychological service.
A referral letter directed to the psychologist by name or may be addressed generically to ‘the psychologist’. According to advice from Medicare, legislation does not require that a referral should be addressed to a named health professional. If a referral is addressed to one provider, the patient is not obliged to go to the same practitioner. The patient can see another practitioner in the same discipline, provided they can provide the same psychological service.
For more information on communication requirements between referrers and providers of mental health services, refer to the Practice guide: Communication between medical and mental health professionals.
Telehealth consultations
A FPS telehealth consultation is an evidence-based psychological service that is delivered via video conference where a visual and audio link has been established between a patient and their treating GP. This includes provision of services that relate to the main components of FPS, such as cognitive behavioural therapy and interpersonal therapy.
Access more information on FPS telehealth consultations.
Access more information on FPS telehealth consultations.
From 1 November 2018, eligible GPs and medical practitioners will be able to deliver FPS via videoconference through the Better Access initiative. This enables eligible patients in rural and remote areas access to the provision of FPS services via video conference.
For more information on the MBS item numbers for FPS telehealth consultations, visit MBS online.
For more information on the MBS item numbers for FPS telehealth consultations, visit MBS online.
Vocationally registered GPs and medical practitioners who have registered with Medicare Australia as a provider of FPS are eligible to provide FPS telehealth consultations. The treating GP or medical practitioner can be located anywhere in Australia and must be more than 15 km by road from the patient.
For more information on becoming a GP provider of FPS, visit the ‘Information for GPs’ page on the website.
For more information on becoming a GP provider of FPS, visit the ‘Information for GPs’ page on the website.
Eligible patients are required to have a GPMHTP, located in Modified Monash Model areas 4 – 7 and no more than 15 km from the GP.
For more information on patient eligibility requirements, visit the Department of Health website.
For more information on patient eligibility requirements, visit the Department of Health website.

Chronic Disease Management (CDM) items
Where a patient has a mental illness as well as significant co-morbidities and complex needs requiring team-based care, the GP is able to use both CDM items and the GP MHTP.
Although a GP is not precluded from managing a patient under both the CDM items and the GP MHTP, the GP should consider whether it is necessary to develop two separate care plans. As a general principle, the creation of multiple plans should be avoided, unless the patient clearly requires an additional care plan for the management of a separate medical condition.
Although a GP is not precluded from managing a patient under both the CDM items and the GP MHTP, the GP should consider whether it is necessary to develop two separate care plans. As a general principle, the creation of multiple plans should be avoided, unless the patient clearly requires an additional care plan for the management of a separate medical condition.
According to the MBS, a patient is eligible for access to CDM items if they have at least one medical condition that has been present (or is likely to be present) for at least six months or is terminal.
Examples of eligible conditions provided, include:
Recent advice from the Department of Human Services clearly states a mental health disorder alone does not allow access to CDM items. The specific advice received is that only where a patient also has a chronic medical condition separate to their mental health condition, may it be appropriate for the patient to be on a CDM plan in addition to a GP MHTP. They cannot be offered sequentially to treat a mental health condition
Examples of eligible conditions provided, include:
|
|
|
|
|
Recent advice from the Department of Human Services clearly states a mental health disorder alone does not allow access to CDM items. The specific advice received is that only where a patient also has a chronic medical condition separate to their mental health condition, may it be appropriate for the patient to be on a CDM plan in addition to a GP MHTP. They cannot be offered sequentially to treat a mental health condition
{kind=link}